Changes in the structure of the heart due to sport
The athlete’s heart gradually adapts to dynamic and intense exercises. They cause both the blood pressure and the volume of the cavities to increase. In order for the heart to adapt, it is necessary, in the first case to lengthen the heart muscle by dilating the cavities, and in the second to thicken the heart muscle (also known as hypertrophy). The set of changes in the shape of the heart in response to changes in pressure or volume, is what is called cardiac remodeling.
Classically, athlete remodeling has been divided into two groups, depending on whether dilatation or hypertrophy predominates. However, in all trained people both types of remodeling appear to a greater or lesser extent.
In the hearts of young athletes, the most frequent (almost 50% of cases) is dilatation and hypertrophy of the right ventricle, with the goal of pumping more non-oxygenated blood to the lungs and obtaining more oxygen back to the left ventricle to be pumped to the body muscles. This is achieved by lengthening, thickening, and increasing the elasticity of the heart muscle.
This way, it is possible to pump much more blood per minute without hardly increasing the pressure inside the cavities. Cardiac remodeling allows the heart to increase the volume of blood that it pumps with each beat, so it needs to beat fewer times per minute to do the same job. In other words, it becomes more efficient.
This affects both ventricles, but in the right ventricle, the change is more visible. In addition, cardiac remodeling is accompanied by an improvement in vascularity so that the heart muscle, better nourished by blood vessels, is more resistant to physical stress.
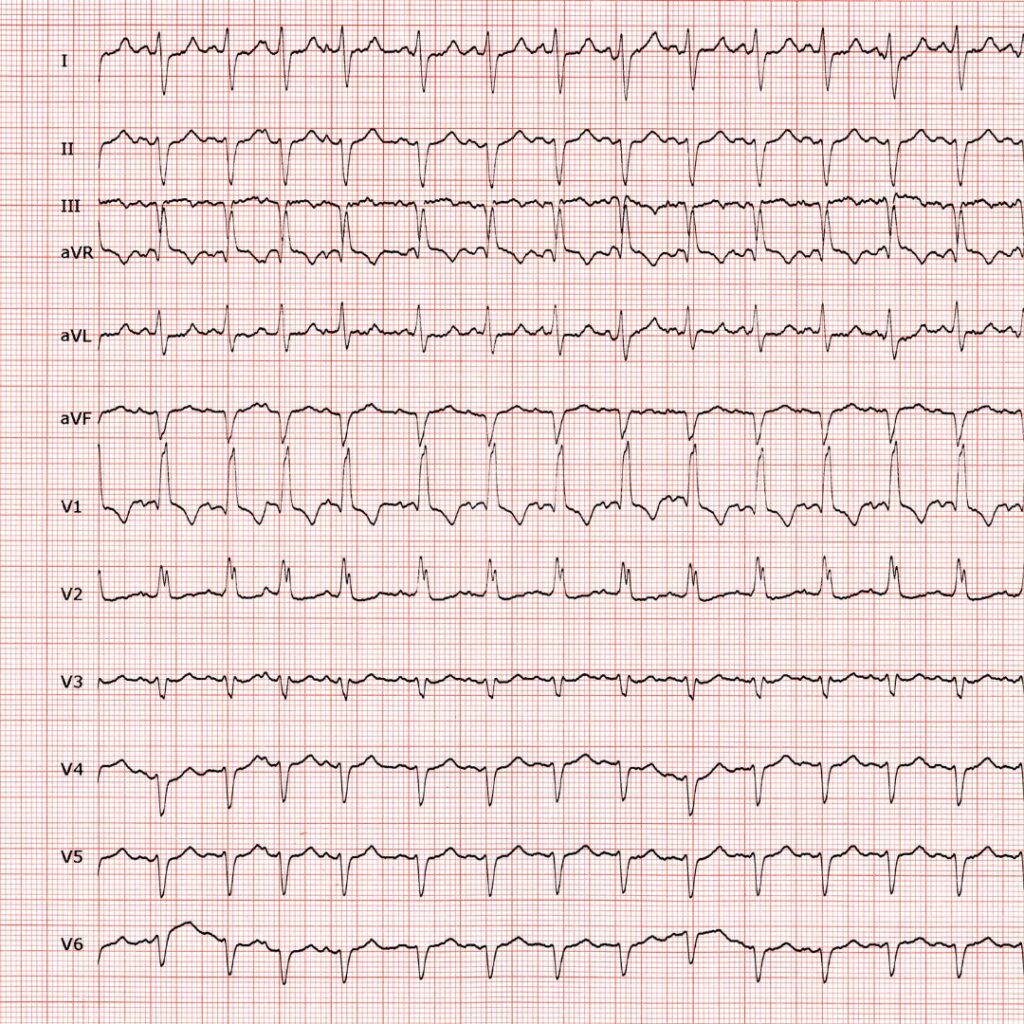
In a practical way, what we see in the electrocardiograms is usually a drop in the heart rate and a lengthening of the ventricular contraction time to around 10 milliseconds or less (more ventricular mass requires more time for the contraction), which in the right ventricle results in the appearance of a second positive wave called the R-prime wave in the ventricular complexes in V1 and V2 (which are the septal leads that explore the right side of the heart). The morphology of the rSR’ complexes that do not exceed 0.12s of contraction time is what is called IRBBB (incomplete right bundle branch block).
Sometimes this phenomenon is less apparent and remains only in small notches in the rising branch of the S wave.
IRBBB is asymptomatic and insignificant. It shows how the heart adapts to the physical stress to become more efficient. Only if it lasts for more than 0.12s (and especially if it reaches 0.14s) can we speak of the complete block (CRBBB), which requires more detailed study with an echocardiogram.
Football players from the Football Federation of Comunidad Valenciana have to pass a medical examination every two years. At Clínica La Siesta, as part of the examination, an electrocardiogram is performed to control the state of health of the heart. Every year, many cases of incomplete right bundle branch block are detected among athletes.